Introduction
The rates of breastfeeding in the U.S. have significantly increased, an estimated 81% of women in the United States attempt to breastfeed during the early life of their baby but cease shortly afterward (CDC, 2016). The Department of Veterans Affairs (2009) noted that approximately 50%-90% of expectant mothers decide how they will feed their babies before conceiving or early in their pregnancy.
There are many factors that impact the mother’s choice to breastfeed or not to breastfeed. Mothers do not initiate breastfeeding because they may view breastfeeding as disgusting or unappealing, whereas bottle feeding may be easier, or they may have a medical condition or the mother may return to work/school. Other breastfeeding mothers cease to breastfeed breastfeeding before 6 months because of perceived low milk supply, or they may state that the child weaned itself, the mother returned to work/school, inconvenience, and fatigue of the mother (Miller & Maclean, 2005). Insufficient milk supply is one of the most common reasons mothers gave as to why they stopped breastfeeding. Research indicates less than 5% of women are physiologically incapable of producing an adequate milk supply (Hector et al. 2005).
There are health disparities found within the breastfeeding population. Age, education, income, neighborhood, as well as cultural ethnicity all, have an impact on breastfeeding rates (Surgeon General Report, 2011). Young mothers are notoriously less likely to start breastfeeding. Only 71% of mothers with a high school education breastfeed compared to 89% of mothers with a college education. Around 74% of women breastfeed in lower-income households compared to 89% in the highest income brackets. Of mothers in rural areas, 80% breastfeed compared to 86% in urban areas. Comparing immigrant mothers, 83% of non-immigrant mothers breastfeed compared to 92% of immigrant mothers (Griffiths et al. 2005).
Literature Review
No previous research has been done on the breastfeeding duration and predictors of breastfeeding continuation and cessation among Women Veterans within Veterans Integrated Service Network (VISN) 15 VA Health Care System. VISN 15 is inclusive of 8 major healthcare facilities and 54 outpatient clinics where Women Veterans are seen for health care. Women Veterans currently make up 6% of VA health care users within VISN 15 (Saint Louis VA Women’s Health Strategic Plan, 2014). Over the next 10 years, all facilities within VISN 15 are going to experience a significant influx of Women Veterans of all ages (increase of 35%), including those of reproductive age (increase of 8.2%), and a decline in the population of male Veterans (decline by 5%) (Defense Manpower & Data Center, 2011).
The increase in women correlates with a greater need for prenatal care. Understanding the changing trends in Women Veterans seeking maternity benefits will help the Veterans Health Administration (VHA) to improve the quality of reproductive care over time. This research will be used to quantify the duration of exclusive breastfeeding among Women Veterans and to understand the predictors of breastfeeding continuation and cessation among VISN 15 sites. The study results may be used to develop targeted prenatal and postnatal breastfeeding education for Women Veterans within VISN 15.
This study is important because there are currently no studies that have exclusively investigated the breastfeeding practices of Women Veterans. Most breastfeeding studies have been conducted among civilian populations, and few studies have assessed breastfeeding trends of active duty or Women Veterans alone. For instance, Martin et al. (2015) examined the perceptions of breastfeeding support among active-duty women who were in the U.S Armed Forces to identify barriers and breastfeeding policies. The findings indicated that active-duty women of low socioeconomic status and women of Hispanic origin had lower scores for breastfeeding support. A survey of 254 active-duty women and military dependents did not meet the successful breastfeeding goals as set by the Academy of Pediatrics because of potential barriers (Bales, Washburn & Bales, 2012). The American Academy of Pediatrics goals for breastfeeding includes the recommendation that infants be exclusively breastfed for about the first 6 months with continued breastfeeding alongside the introduction of appropriate complementary foods for 1 year or longer. Similarly, a different study of 253 uniformed families that was compared to national data of breastfeeding women showed that uniformed women initiated and continued to breastfeed at a slightly higher rate than civilian women, however, the breastfeeding rates of military women were also less than the standards set by the American Academy of Pediatrics (Mao et al. 2012). Another study compared breastfeeding health disparities among black and white “military-affiliated” women by using a retrospective study design that was based on the CDC’s PRAMS (Pregnancy Risk Assessment Monitoring System). “Military affiliated” mothers included active duty wives, spouses, and daughters, and the study did not make any distinctions between active duty, dependents, or Women Veterans (Lundquist & Barfield, 2015). As these studies point out, breastfeeding research was conducted in “military-affiliated” women, however, studies were either unclear or silent on the breastfeeding rates and experiences of exclusively Women Veterans. Given the gap in the literature, this study will expand the breastfeeding literature by examining the duration and predictors of breastfeeding of Women Veterans.
A review of 110 studies supports the effectiveness of breastfeeding education for increasing breastfeeding rates (Haroon et al. 2013). Studies assessed included individual counseling, group counseling, and a combination of both. Compared to no intervention, breastfeeding instruction increased exclusive breastfeeding rates at one month postpartum by 43% and at 1-5 months by 90%. Providing education was also linked to decreased rates of women choosing not to breastfeed. While all interventions increased breastfeeding rates, types that used combined individual and group counseling produced the most significant effects (Haroon et al. 2013). Another review of breastfeeding education found that both pre- and postnatal interventions have a significant impact on breastfeeding rates. Data showed that in developed countries when education was given the exclusive breastfeeding rate at six months postpartum increased by 30% compared to no intervention (Imdad, Yakoob & Bhutta, 2011).
Maternity benefits have been included in the VHA medical benefits package since 1996. All maternity care within VISN 15 is provided by community obstetrical providers through the VHA fee-basis care program (Mottocks, et al. 2014). It is a specific VA and Department of Defense policy to offer breastfeeding education to all pregnant women during the first visit with a provider. It is up to the provider to use open-ended questions to encourage breastfeeding. The recommendation is to ask pregnant women, “What do you know about breastfeeding?” rather than, “Do you plan on breast or bottle feeding” to provide an open opportunity for education. Prenatal breastfeeding education should be continued throughout pregnancy for all women regardless of their decision of infant feeding method, however, this is a barrier as Women Veterans receive their maternity care through a Non- VA obstetrician, who may or may not provide breastfeeding information during prenatal visits. There are many recommendations to include family/significant others in breastfeeding education to build a network of support for the mother after delivery (Department of Veterans Affairs, 2009). VA supports breastfeeding by providing Women Veterans with a maternity belt, breast pumps, and nursing bras through a prosthetics consult at least 2 weeks in advance of the Veteran’s estimated date of delivery. Related supplies, such as breast pads and nipple cream, may be obtained through the VA Pharmacy (Department of Veterans Affairs, 2012).
The increase in Women Veterans of reproductive age within VISN 15 over the next 10 years correlates with a greater need for prenatal care. Understanding the changing trends in Women Veterans seeking maternity benefits will help the VHA to improve the quality of reproductive care over time. Even while all maternity care is provided by community obstetrical providers through the VHA fee-basis care program (Mottocks, et al. 2014), there is a need for breastfeeding support pre- and postnatally for Women Veterans, who will return to their VA Primary Care Clinics after delivery. The research will be used to quantify the duration of exclusive breastfeeding among Women Veterans and to understand the predictors of breastfeeding continuation and cessation. The study results may be used to develop targeted prenatal and postnatal breastfeeding education for Women Veterans within VISN 15.
This study is important because there are currently no studies that have exclusively investigated the breastfeeding practices of Women Veterans. While most breastfeeding studies have been conducted among civilian populations, there is a scarcity of literature that examines the duration, or continuation of breastfeeding among Women Veterans. There are few studies that have assessed breastfeeding trends of active duty and Women Veterans exclusively. Studies generally make no distinction between military or dependents, referring to these women as “military-affiliated women.” For active-duty military women and Women Veterans, there may be distinct differences in the attitudes and skills for breastfeeding infants compared to the civilian population.
Theoretical Framework
The theoretical framework used in this study is the Theory of Planned Behavior (TPB). TPB has been used in breastfeeding studies that examine breastfeeding duration with maternal intention and correlated with self-efficacy (Lau, Lok & Tarrant, 2018). This theory hypothesizes that human action is guided by three kinds of consideration: behavioral beliefs (beliefs about the likely consequences of the behavior), normative beliefs (beliefs about the normative expectation of others) and control beliefs (beliefs about the presence of factors that may facilitate or impede performance of the behavior) (Azjen 2002). Essentially, the more favorable the attitude and subjective norms and the greater the perceived control, the stronger the person’s intention to perform the behavior in question.
Research Questions
There were five questions that guided this study.
- What are the breastfeeding intentions of Women Veterans in VISN 15?
- What is the breastfeeding duration of Women Veterans in VISN 15?
- What are the positive factors that contribute to breastfeeding continuation of women Veterans in VISN 15?
- What are the negative factors that contribute to breastfeeding cessation among women Veterans in VISN 15?
- What is the breastfeeding knowledge and understanding of breastfeeding services by the VISN 15 Women’s Health Care Services among Women Veterans?
Methods
Research Design
This research used a cross-sectional study design. This type of design took measures of a sample at a single point in time and did not conduct any follow-up (Sedgwick, 2014). Further, a cross-sectional design was ideal when capturing the prevalence of behavior by utilizing a questionnaire survey. Given that this was the first time that a breastfeeding study was scaled up among exclusively Women Veterans, a cross-sectional design offered the ability to better understand the duration and predictors related to this group.
Data Collection Procedures
Data collection took place from September 2016 after IRB and DART approval. A contact list of Women Veterans who gave birth to live infants between January 1, 2014, and August 31, 2016, was provided by VA Informatics and Computing Infrastructure (VINCI) workspace. The contact list had approximately 900 Women Veterans based on the numbers provided by the Women’s Health Program Managers at the eight VISN 15 sites. The requested information from VINCI was comprised of names, social security numbers, addresses and telephone numbers. After DART approval a letter was mailed to all identified Women Veterans within VISN 15 inviting them to participate in the survey. This letter was followed by a telephone call. During the telephone call, the Women Veteran was asked for verbal consent to respond to a telephone survey about their breastfeeding duration and experiences. Some Women Veterans opted not to respond to the survey by either not returning the call or by verbally informing the investigator they did not wish to participate. No further contact was attempted with the Women Veterans who refused survey participation. For those who agreed to continue with the telephone survey, study questions were asked by the principal investigator or intern.
Results
Descriptive analysis was conducted using excel. The first part provides some demographic features of the fifty-six Women Veterans who responded to the survey. The second part presents the findings based on the research questions posed.
Demographic Information
The age range of respondents ranged between 18-45 years, the majority of the women were between the ages of 26-35 (66.07%, M =2.3, SD=0.61). Five percent (5.36%) of the respondents refused to endorse income level, most of the respondent’s income level ranged between $25,000-$50,000 (35.71%, M=2.9, SD=0.17). The number of respondents who stated income levels between $50,000-$75,000, was 30.36% ( M= 2.9, SD=1.79). Only 8.9% of the new mothers stated their income level was < $25,000, while 19.64% stated income levels above $75,000. In relation to education, the mean was M=2.8, and the SD=0.091. Most of the respondents (57.14%) had a college degree, while 14.29% had a post-graduate degree. Table 1 and 2 detail the demographic summaries of the Women Veterans.
Table 1. Demographic Features of the Women Veterans
| Age | n | % |
| 18-25 | 1 | 1.7 |
| 26-35 | 37 | 66 |
| 36-45 | 17 | 30 |
| Other | 1 | 1.7 |
| Income | ||
| <$25,000 | 5 | 8.6 |
| $25,000-$50,000 | 20 | 35.7 |
| $50,000-$75,000 | 17 | 30 |
| $75,000-100,000 | 4 | 7 |
| >$100,000 | 7 | 12 |
| Refused to answer | 3 | 5 |
| Education | ||
| HS/GED | 1 | 1.7 |
| Some College
College Degree Grad Degree Total # of Participants |
15
32 8 56 |
26.7
57.1 14.2 100
|
The largest group of respondents (57.14%) were Caucasian, 14.29% Hispanic, 19.64% Black and 8.93% other.
Table 2: Ethnic Background of Women Veterans
| Ethnicity | n | % |
| Hispanic | 8 | 14 |
| White | 32 | 57 |
| Black | 11 | 19 |
| Other | 5 | 8.9 |
RQ1. What are the breastfeeding intentions of Women Veterans?
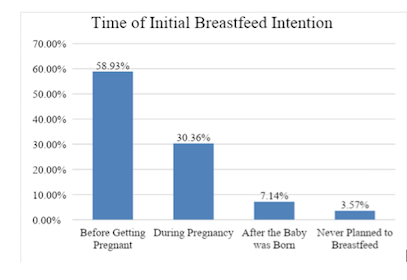
Most of the Women Veterans who breastfed their infants (58.93%) planned to breastfeed prior to becoming pregnant. The second highest group (30.36%) of women planned to breastfeed during pregnancy. There were fewer (7.14%) women who decided to breastfeed after the birth of their child, with 3.5 % reporting that they never planned to breastfeed.
Figure 1. Date of Initial Breastfeeding Intention
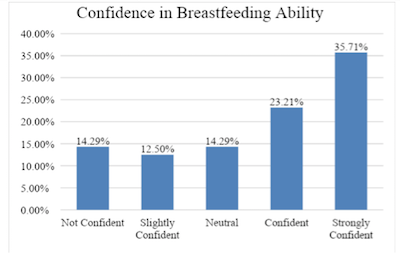
Most of the respondents felt they had the necessary skills to breastfeed, 23.21 % reported being confident at breastfeeding and 35.71% stating that they were strongly confident in their ability to breastfeed as shown in figure 2.
Figure 2. Confidence in Breastfeeding Ability
In terms of the ease of breastfeeding, an equal number of 25% of the Veteran Women indicated that breastfeeding was not easy and the other reported that it was easy.
Figure 3. Reported Ease of Breastfeeding

RQ2. What is the breastfeeding duration of Women Veterans in VISN 15?
Most of the Veteran Women (30.36%) were still breastfeeding at the time of this study. Thirty-four percent (34%) of the Women Veterans stopped breastfeeding after more than 12 months, followed by 18 % of women who stopped breastfeeding when their babies were between 3-6 months. Fourteen percent (14%) quit breastfeeding when the baby was 6-9 months. For most new mothers who stopped breastfeeding, 32.14% started formula between the infant ages of 6-9 months. Twenty percent introduced formula when their infants were 3-6 months.
RQ3. What are the positive factors that contribute to breastfeeding continuation?
When asked if the respondents had support from their partner, mother and doctor to breastfeed, there was a positive trend of support. Eighty two percent (82%) of Women Veterans strongly agreed that their spouse supported their breastfeeding; 71% and 89% also strongly agreed that their mother and doctor supported their breastfeeding respectively.
RQ4. What are the negative factors that contribute to breastfeeding cessation?
The most common reason negative factors for discontinuation of breastfeeding among 30% of the Women Veterans was that they were not producing enough breast milk. The second reason among 24% was considered under “other,” a review of the women’s reasons included being out in public, baby going to daycare, and being inexperienced. The third factor was returning to work for 18% of the women and 10% women indicated that their baby seemed hungry.
RQ.5. What is the breastfeeding knowledge and understanding of breastfeeding services by the VISN 15 Women’s Health Care Services among Women Veterans?
About half of the Women Veterans surveyed (53.57%) stated that the VA provided breastfeeding information to them, and most (73.21%) were aware that the VA would provide a breast pump. Additionally, the majority (71.43%) expressed support for breastfeeding after birth by VA personnel.
Discussion
This study reveals some key areas that continue to be a work in progress and some that confirm the breastfeeding literature. Based on the theory of Planned Behavior (TRB) this study confirms that more participants intended to breastfeed before they delivered their baby, and some decided during their pregnancy. In addition, some of the Women Veterans were confident in their ability to breastfeed, some were not. They also reported that breastfeeding was socially supported by their partners, their mothers, and their physicians, confirming that the subjective norms of breastfeeding were largely supported by the Women Veterans’ support networks. This finding was one of the strengths of this study because it provided some insights into why some Women Veterans continued to breastfeed. The literature confirms that when women have a firm support system either from their partners (Persad & Mensinger, 2007 & Mahesh et al. 2018) or from the healthcare professionals (Johnston & Esposito, 2007) the likelihood of mothers’ to breastfeed increases.
On the other hand, the perceived behavioral control i.e the skill of breastfeeding was not considered easy by 25% of the Women Veterans. Whereas, 16 % reported being neutral about their breastfeeding skill. This finding speaks to the challenges that some breastfeeding mothers experience. Brown’s (2016) study reported that breastfeeding women preferred messages that acknowledged the realities of breastfeeding, specifically, she indicated that women “need realistic information about what breastfeeding. In Brown’s (2016) study, women felt unprepared for what it was like, or they felt they were doing it wrong after birth, or they felt disillusioned and misled, and needed information on how to deal with the difficulties” (p.105). The breastfeeding challenges could be addressed with pre and postnatal breastfeeding interventions that are critical in building breastfeeding skill among Women Veterans.
Based on the World Health Organization (WHO, 2019) breastfeeding recommendations, infants should breastfeed exclusively for 6 months. Some of the Women Veterans (20%) in this study started supplementing with formula when their babies were between 3-6 months instead of following the WHO recommendation. Further, the Surgeon General’s Call for exclusive breastfeeding 2020 objectives were targeted at 46% for 3 months and 25% exclusive breastfeeding for infants who are breastfed at 6 months (Healthypeople.gov). Even though there was a sizable group of Women Veterans who intended to breastfeed before or during pregnancy in this study, the actual number of women who breastfed was not the same as those who reported intention. This finding confirms the complexity of breastfeeding intention and the act of breastfeeding affects most women including Women Veterans.
Overall, this study confirms that the Women Veterans are aware of the breastfeeding resources. However, gaps still remain related to the duration of breastfeeding, ease of breastfeeding, confidence and the negative factors that contributed to breastfeeding cessation among some Women Veterans.
Limitations and Recommendations of the Study
The small number of respondents in this study was a major limitation of the study. The study was not a randomized study, therefore, the findings are not generalizable to other Women Veterans in different VISNS. Since there was a limited number of participants who responded to our phone calls, we recommend a close examination of an updated VINCI database. We recommend enrolling (through face-to-face) a larger group of Women Veterans if a quantitative study is considered on breastfeeding. In addition, it might be worth comparing Women Veteran’s breastfeeding behavior and the predictors of breastfeeding continuation and cessation to civilian women. Such a study should be coupled with a qualitative design so that more in-depth insights into the fears and reasons for breastfeeding among Women Veterans are explored.
Conclusion and Practical Implications
This study was an “in-house” study which added to the gap in the military breastfeeding literature among Women Veterans. It sheds some insights into understanding the breastfeeding duration and predictors of breastfeeding continuation and cessation. Women Veterans remain an underrepresented group in all research, including the survey of their attitudes about their healthcare throughout the reproductive life cycle. By analyzing specific results focused on Women Veterans, the Veterans Health Administration (VHA) will be able to provide improved and successful interventions to support Women Veterans and their families. Improved breastfeeding support within the VHA may include employment of lactation coaches, educator, or other specialists to assist in the management of breastfeeding skill and confidence surrounding breastfeeding for new mothers.
References:
Bales, K., Washburn, J., & Bales, J. (2012). Breastfeeding rates and factors related to cessation in a military population. Breastfeeding Medicine 7(6):436-441.
Boston University Medical Campus. (2012). Recruitment letter template. Clinical Research Resources Office. Retrieved http://www.bumc.bu.edu/crro/recruitment/resources/letters/
Brown, A. (2016). What do women really want? Lessons from a breastfeeding health promotion and education. Breastfeeding Medicine,11(3),102-110. doi.org/10.1089/bfm.2015.0175
Centers for Disease Control (2014). Breastfeeding Report Card – United States. National Center for Chronic Disease Prevention and Health Promotion/Division of Nutrition, Physical Activity, and Obesity; 2014:1-8. Retrieved from http://www.cdc.gov/breastfeeding/pdf/2014breastfeedingreportcard.pdf.
Centers for Disease Control. (2016). Breastfeeding continues to rise. Retrieved from https://www.cdc.gov/media/releases/2016/p0822-breastfeeding-rates.html
Department of Veterans Affairs – Department of Defense. (2009). VA/DoD clinical practice guideline for pregnancy management. Department of Veterans Affairs – Department of Defense. Retrieved from http://www.healthquality.va.gov/guidelines/WH/up/mpg_v2_1_full.pdf.
Department of Veterans Affairs. (2012). Maternity health care and coordination. VHA Handbook 1330.03. 2012. Retrieved from http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2803.
Defense Manpower and Data Center. (2011, April). Unpublished data as of 30 September 2010. Compiled by the Women’s Research & Education Center. Retrieved from http://www.womenshealth.va.gov/womenshealth/docs/women_veterans_healthcare_factsheet.pdf
Gartner, L.M. , Morton, J. , Lawrence, R.A. , Naylor, A.J. , O’Hare, D., Schanler, R.J ., & Eidelman, A. I. (2004). Breastfeeding and the use of human milk. Pediatrics. 115(2):496-506.
Griffiths, L. J., Tate, R. A. & Dezateux, C. (2005). The contribution of parental and community ethnicity to breastfeeding practices: evidence from the Millennium Cohort Study. International Journal of Epidemiology, 34(6):1378-1386.
Haroon, S., Das, J.K., Salam, R.A., Imdad, A., & Bhutta, Z.A. (2013). Breastfeeding promotion interventions and breastfeeding practices: A systematic review. BMC Public Health, 13 (3) S20.
Haque, F., Mills, M., & Corstorphine, N. (2005). Breastfeeding Survey Report. 1st ed. Timmins: Porcupine Health Unit:17-30. Retrieved from http://www.porcupinehu.on.ca/Reports/documents/2005BreastfeedingSurveyReport.pdf
Healthypeople.gov. (2019). Breastfeeding. Retrieved from https://www.healthypeople.gov/
Hector, D., King, L., Webb, K., & Heywood, P. (2005). Factors affecting breastfeeding practices. Applying a conceptual framework. NSW Public Health Bulletin, 16(4), 52-55.
Imdad, A., Yakoob, M.Y., & Bhutta, Z.A. (2011). Effect of breastfeeding promotion intervention on breastfeeding rates, with special focus on developing countries. BMC Public Health. 2011, 11(3), S24. http.//www.biomedcentral.com/14712458/11/S3/S24.
Johnston M. L., & Esposito, N. (2007). Barriers and facilitators for breastfeeding among working women in the United States. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 36(1), 9–20.
Lindquist, J., Xu, Z., & Barfield W. (2015). Do black and white racial disparities in breastfeeding persist in the military community? Maternal Child Health Journal, 19, (2), 419-427.
Lau, C.Y.K., Lok, K. Y. W., Tarrant, M. (2018). Breastfeeding duration and the theory of
planned behavior and breastfeeding self-efficacy framework: a systematic review of observational studies. Maternal Child Health Journal, 22(3), 327-342. doi: 10.1007/s10995-018-2453.
Mahesh, P., Gunathunga, M. W., Arnold, S. M., Jayasinghe, C., Pathirana, S., Makarim, M. F., …
Senanayake, S. J. (2018). Effectiveness of targeting fathers for breastfeeding promotion: systematic review and meta-analysis. BMC Public Health, 18(1), 1140. doi:10.1186/s12889-018-6037.
Mattocks, K.M., Frayne, S., Phibbs, C.S, et al. (2014). Five-year trends in women veterans’ use of VA maternity benefits, 2008-2012. Women’s Health Issues, 24 (1), e37-42.
Mao, C.Y., Narang, S., & Lopreiato, J. (2012). Breastfeeding practices in military families: A 12-month prospective population based study in the national capital. Military Medicine, 177(2), 229-234.
Millar, W., & Maclean, H. (2005). Breastfeeding Practices. Ottawa: Statistics Canada; 2005:23-34. Retrieved from http://publications.gc.ca/Collection-R/Statcan/82-003-XIE/0020482-003-XIE.pdf.
Persad M., & Mensinger J. L. (2007). Maternal breastfeeding attitudes: Association with breastfeeding intent and socio-demographics among urban primiparas. Journal of Community Health, 33, 53–60.
Siedwick, P. (2014). Cross-sectional studies: advantages and disadvantages. British Medical Journal, 348, 2276. doi: http://dx.doi.org/10.1136/bmj.g2276
U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Support Breastfeeding. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2011.
World Health Organization. (2019). Breastfeeding. Retrieved from https://www.who.int/nutrition/topics/exclusive_breastfeeding/en/

